
Hypoxia & Hyper-coagulability
Oxygen saturation:

Terminology:
SpO2:
- hemoglobin saturation, normal is 100%
- Measured via pulsoximeter (inaccurate in CO poisoning and with vasoconstriction of the fingers)
PaO2:
- partial pressure of oxygen in the arterial blood, normal is 90-100mmHg
- Measured via arterial blood gas measurement
Causes of low oxygen saturation:
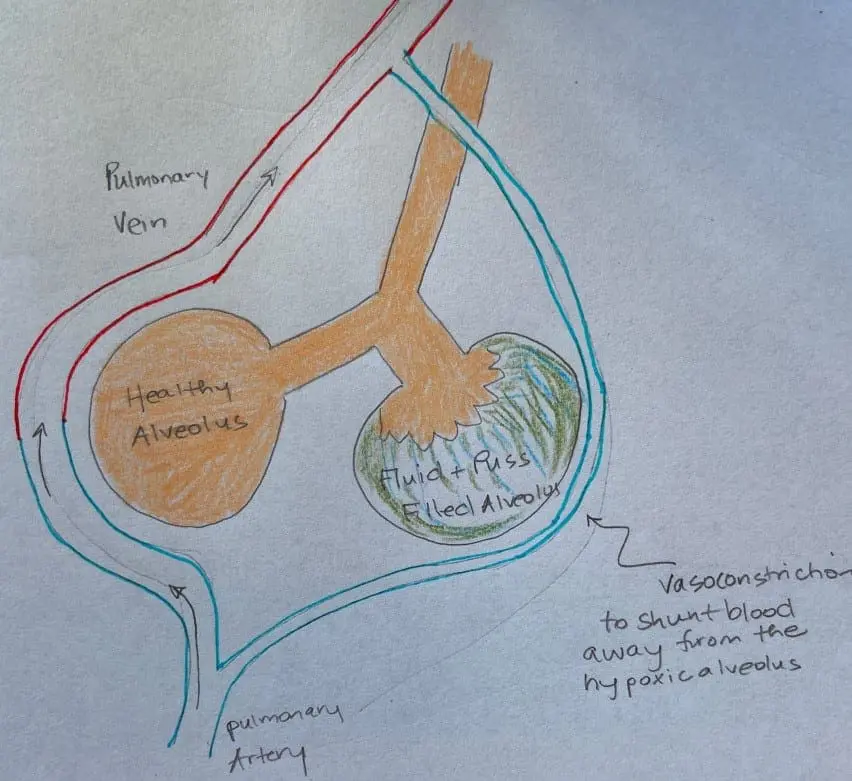
- Poor ventilation: fluid and puss blocking the diffusion of oxygen from the alveoli to the capillaries
- Poor perfusion: vasoconstriction of the capillaries or blockage of the capillaries by a clot
- Defects in hemoglobin binding affinity due to low oxygen saturation or other unidentified defect (heme synthesis defect? Subclinical porphyria? methemoglobin?)
Hemoglobin (Hgb):
4 binding domains for oxygen
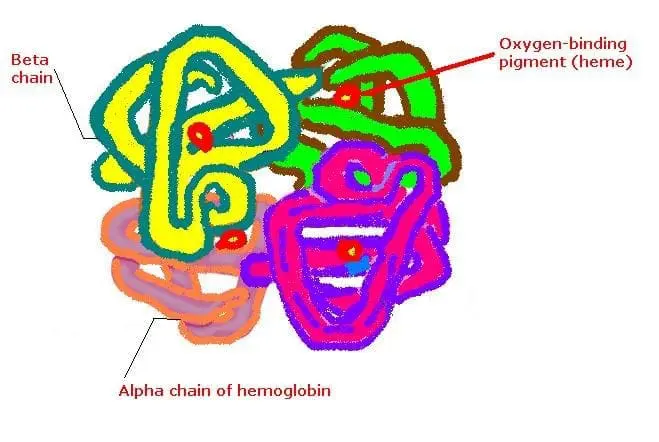
Binding affinity:
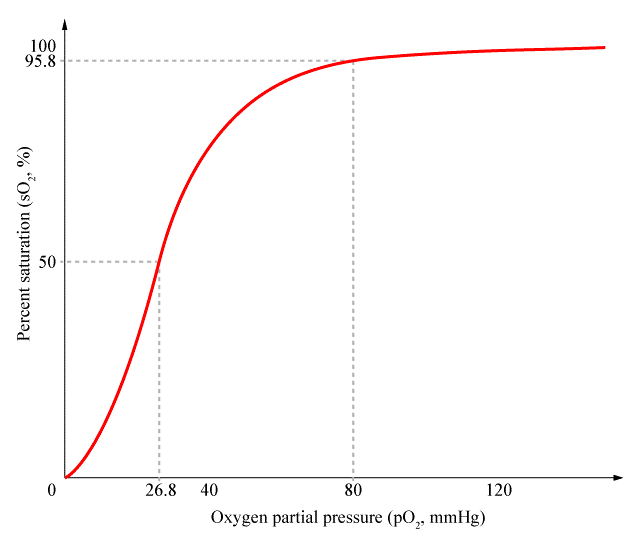
– Increases with each bound hgb molecule until all 4 are bound, to encourage the hgb to pick up all four oxygen molecules in the lungs
– Decreases in areas of low oxygen pressure (enhances dissociation in hypoxic tissue), rapid drop at 90% saturation or less

Poor perfusion:
- Vasoconstriction:
-
- Hypoxic pulmonary vasoconstriction (HPV): vasoconstriction of the pulmonary artery supplying a defective alveoli. Bypasses this part of the lung.
- High altitude, pulmonary edema (HAPE): If in a low oxygen environment, the pulmonary artery vasoconstricts globally, increasing pulmonary artery pressure. The increased pressure can cause rupture of the pulmonary artery capillaries allowing fluid to leak into the alveoli. Can this occur due to the severe hypoxia induced in COVID-19?
- High levels of Angiotensin-II, a potent vasoconstrictor. Is this due to the virus inhibiting ACE2?
- Microthrombi:
- Small clots blocking capillaries in the lungs leading to rupture and leaking of fluid into the lungs. These clots cause ischemia in other areas of the body including the brain, organs and extremities leading to stroke, organ failure and necrosis.
What is the cause of hyper-coagulability in COVID-19:
Disseminated Intravascular Coagulation (DIC):
- 4% of patients who die of COVID-19 meet ISTH criteria for DIC
- Increased IL-6—> damage to endothelium—> consumption of platelets and Increased PAI-1 (inhibits fibrinolysis)—>micro (renal, cardiac, pulmonary) and macro (PE, DVT) thrombosis
NOTE: One group of authors found that typical DIC criteria were not met in their patient group, suggesting another explanation for the hyper-coagulability (no reduced platelet count or change in prothrombin time or activated partial thromboplastin time).
Another explanation: Anticardiolipin IgA and anti-β2-glycoprotein I IgA and IgG:
- These are antibodies that attack the phospholipids of cell membranes. They form in response to the infection. We commonly see these antibodies triggered by the tick-born pathogen Bartonella.
- They bind to and lead to damage by immune attack of the endothelial cell membrane, stimulating clotting.
Interventions:
The International Society on Thrombosis and Haemostasis recently recommended that all hospitalized COVID-19 patients, even those not in the ICU, should get prophylactic-dose low molecular weight heparin (LMWH), unless they have contraindications (active bleeding and platelet count <25×109/L).
Recommendations from Britain also call for venous thromboembolism prophylaxis for all high-risk patients as well as considering pulmonary embolism for patients with sudden onset of oxygenation deterioration, respiratory distress, and reduced blood pressure.
Indications to start anticoagulants:
- D-dimer >1,500 ng/mL
- fibrinogen >800 mg/mL
Anticoagulant therapy was more successful for patients with:
- sepsis induced coagulopathy (SIC) criteria ≥4
- markedly elevated D-dimer (greater than six-fold at the upper limit of normal)
Options for thromboprophylaxis (preventing clotting):
Anticoagulants (prevent formation of clots but do not break them down):
- IV unfractionated heparin: can be stopped easily, anti-inflammatory
- IV low molecular weight heparin (LMWH): 40 – 60mg/day, 0.6mg/kg per 12hrs for 7d or longer
- Enoxaparin: 1 mg kg s/c q 12 hours (dose adjust with Cr Cl < 30mls/min)
- Oral anticoagulants or vitamin K antagonists
- In patients with a history of heparin-induced thrombocytopenia (HIT) use fondaparinux
Thrombolytic (break down formed clots):
- Tissue plasminogen activator (Alteplase): 25mg of tPA over 2 hours followed by a 25mg tPA infusion administered over the subsequent 22 hours, with a dose not to exceed 0.9 mg/kg followed by full anticoagulation with heparin drip.
Monitoring on anticoagulant therapy:
If bleeding:
- Keep platelets count >50
- Fibrinogen> 2g/L
If not bleeding:
- Keep platelets count >20
- Fibrinogen> 2g/L
- PT ratio <1.5
Contraindications:
- Active bleeding
- Platelet count <25×109/L
- Monitoring advised in severe renal impairment
- Abnormal PT or aPTT is not a contraindication
Natural anti-coagulation methods to consider pre-infection:
- Nattokinase or other proteolytic enzymes 60 minutes before meals
- The juice of one whole lemon (crushed by a juicer) in water daily
- Optimal hydration: 1/2 your body weight in ounces of water per day
- Minimize exposure to EMF (EMF is a possible promoter of clotting): unplug wifi at night, unplug lamps and other electronics at night, keep cell phone on airplane mode when not in use, consider grounding mats for your bed
References:
https://www.ncbi.nlm.nih.gov/pubmed/32268022
https://www.ncbi.nlm.nih.gov/pubmed/32267998
https://www.medpagetoday.com/infectiousdisease/covid19/85865
https://www.medpagetoday.com/infectiousdisease/covid19/85865
https://www.ncbi.nlm.nih.gov/pubmed/32220112
https://www.ncbi.nlm.nih.gov/pubmed/32267998
https://airwayjedi.com/2015/12/09/difference-oxygen-saturation-pao2/